Targeting dormant tumor cells to prevent recurrent breast cancer: a randomized phase 2 trial
Breast cancer is the most common cancer in women worldwide, and while detection of early-stage disease is largely curable, between 20-30% of patients will relapse to develop distant, incurable, metastatic disease years, or even decades, following successful treatment.
February 26, 2026
Introduction
Breast cancer is the most common cancer in women worldwide, and while detection of early-stage disease is largely curable, between 20-30% of patients will relapse to develop distant, incurable, metastatic disease years, or even decades, following successful treatment. Breast cancer is divided based on molecular characteristics of the tumor: PR+/ER+ or luminal breast cancer, HER2+ subtype, and triple negative breast cancer (TNBC), which lacks PR, ER, and HER2. These molecular profiles determine treatment regime1.
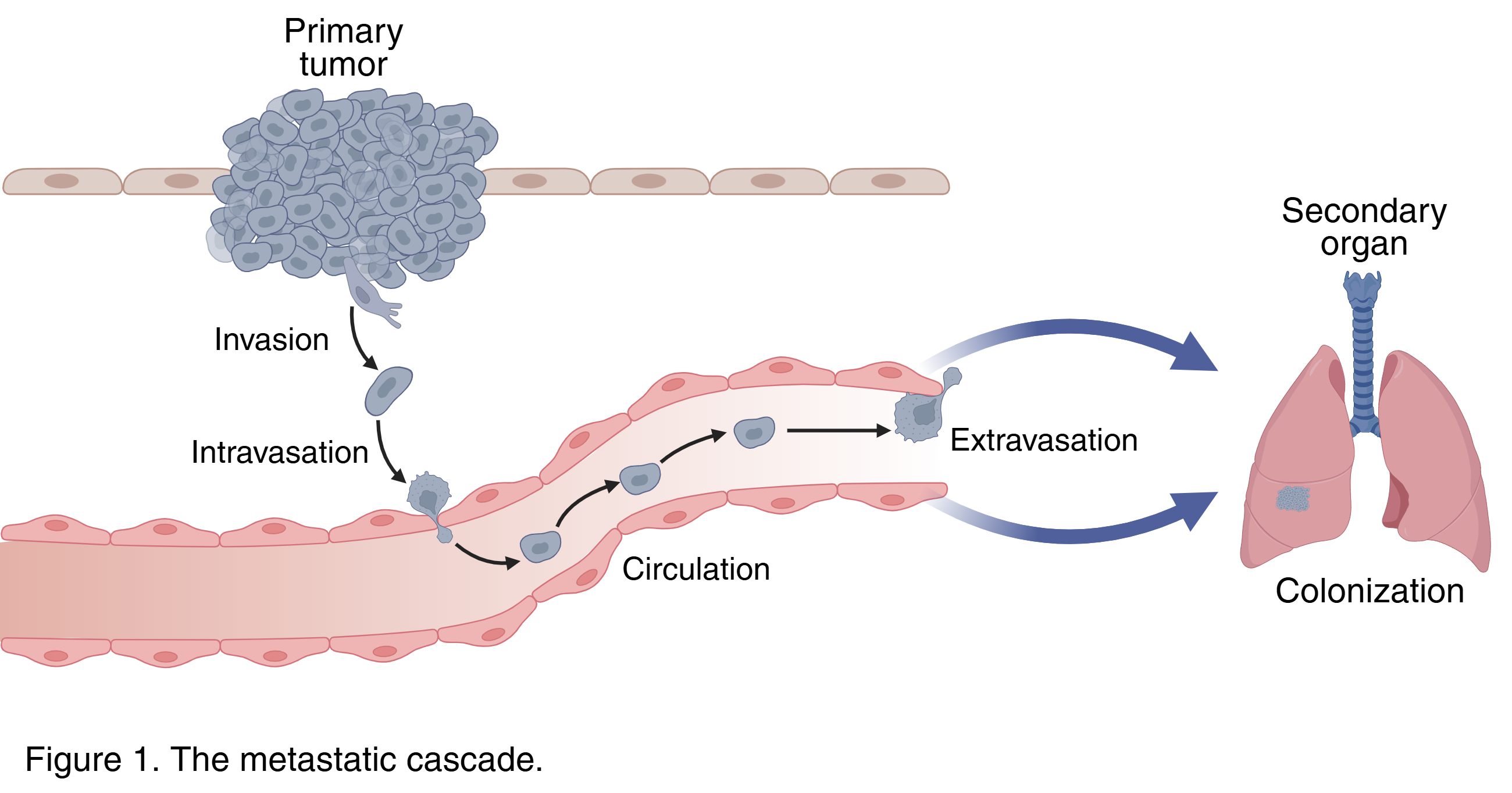
Metastasis is a complex and inefficient process that generally follows a series of steps of distant spread: dissemination from the primary tumor site, survival in circulation, and metastatic outgrowth at a secondary organ. A key feature of breast cancer metastatic seeding is the persistence of residual dormant cancer cells that can remain in a quiescent state for years before disease relapse and distant metastases. Although the biology of dormant tumor cells is not completely understood, recent preclinical studies suggest that alterations in the mammalian target of rapamycin (mTOR), a regulator of autophagy, a catabolic process that is activated in response to stress such as a foreign environment the disseminated tumor cells encounter, are potential mechanisms that promote the survival of dormant residual tumor cells.
Goals of this study
This study builds upon previous work by the same researchers identifying the role of autophagy as a survival mechanism for disseminated dormant tumor cells. In this study, the authors were able to start with preclinical studies that built rationale that progressed into a phase II clinical trial. Specifically, they asked:
Can these residual dormant breast cancer cells be therapeutically targeted to prevent tumor recurrence?
Can these findings be translated into human patients with detectable dormant tumor cells in their bone marrow as an intervention to prevent later disease recurrence?
To model tumor dormancy and recurrence, the researchers utilized a HER2-inducible mouse model. HER2 expression is induced in response to doxycycline. These tumor cells are implanted into the mammary fat pad of mice on doxycycline, and withdrawal of doxycycline results in reduced primary tumor growth that leaves behind a small pool of residual tumor cells (RTCs). These RTCs remain in a dormant state and can spontaneously recur. With this model, they first asked if blocking mTOR, which would activate autophagy, would accelerate tumor recurrence. Surprisingly, treatment with the mTOR inhibitor rapamycin (RAPA) delayed tumor recurrence in these mice.
To better translate these findings with drugs that exhibit less toxicity in the clinic, they then treated mice with hydroxychloroquine (HCQ) and everolimus (EVE) alone or in combination. Chronic inhibition of these pathways delayed tumor recurrence and metastatic outgrowth in the mice harboring RTCs. Furthermore, compared to vehicle control, chloroquine, and HCQ arms, mice treated with RAPA, EVE, or HCQ + EVE exhibited similar numbers of RTCs at 3 weeks and 9 weeks, suggesting that these treatments suppress RTC recurrence and prolong regression free survival (RFS) in these mice.
The preclinical findings provided the rationale for the CLEVER trial, which enrolled 53 breast cancer survivors with detectable dormant tumor cells identified within the previous five years. Patients were randomized to receive six 28-day cycles of HCQ (15), EVE (15), or the combination of HCQ + EVE (8) therapy.
At the three-month time point, reductions in disseminated tumor cells (DTCs) were observed in 80%, 78%, and 87% of patients treated with HCQ, EVE, and HCQ + EVE, respectively. At later time points, DTC reduction exceeded 90% across all treatment arms. At three years of follow-up, RFS was 92% for HCQ, 93% for EVE, and 100% for combination therapy. Overall, the treatments were generally well tolerated.
This study has several notable strengths. The use of a biologically relevant mouse model strengthened the rationale for clinical translation, and the dormancy mechanisms identified appear broadly applicable across breast cancer subtypes. Additionally, the use of FDA-approved drugs enhances the feasibility of this therapeutic approach.
However, the lack of a placebo control arm limits interpretation of recurrence rates relative to standard of care. Furthermore, while immunohistochemistry remains the gold standard for detecting dormant tumor cells, its limited sensitivity highlights the need for more robust and precise assays to accurately measure therapeutic responses when targeting this rare cell population.
Article title: “Targeting dormant tumor cells to prevent recurrent breast cancer: a randomized phase 2 trial.”
Article Reference: DeMichele, A., Clark, A.S., Shea, E. et al. Targeting dormant tumor cells to prevent recurrent breast cancer: a randomized phase 2 trial. Nat Med 31, 3464–3474 (2025). https://doi.org/10.1038/s41591-025-03877-3
Additional references
Banys-Paluchowski M, Reinhardt F, Fehm T. Disseminated Tumor Cells and Dormancy in Breast Cancer Progression. Adv Exp Med Biol. 2020; 1220:35-43. doi: 10.1007/978-3-030-35805-1_3. PMID: 32304078.